



INTRODUCTION
Extensive research during recent years has been conducted to assess the effects of air pollution on population morbidity and mortality. Outdoor and indoor pollutants include but are not limited to particulate matter (PM), ozone (O3), sulfur dioxide (SO2), nitrogen dioxide (NO2), carbon monoxide (CO), lead (Pb), asbestos, and biological pollutants1. Health effects vary according to the type of inhaled pollutants and include vascular diseases, ischemic heart disease, bladder cancer, and respiratory diseases1-4.
According to the World Health Organization (WHO), air pollution affects different aspects of health at even lower concentrations than previously thought5. In addition, some populations are at higher risk to the health impacts of air pollution as poverty is strongly associated with the adverse impacts of household air pollutants5. The main pollutants in high-income countries include O3, PM2.5, NO2, CO, Pb, polycyclic aromatic hydrocarbons (PAHs), and volatile organic compounds (VOCs), while PM2.5, CO, SO2, VOCs, and radon, are primary sources of air pollution in low-middle-income countries5.
Exposure to high levels of air pollutants is particularly harmful to people with chronic lung disease and can lead to symptoms such as coughing and wheezing, chest pain, and irritation of the eyes, nose, and throat that disrupt everyday activity1,2,6,7. The most common chronic respiratory diseases (CRDs) are chronic obstructive pulmonary disease (COPD), asthma, occupational lung diseases, and pulmonary hypertension (PAH).
Poor air quality has been associated with adverse health impacts on children, and prenatal exposure to air pollution is thought to contribute to adverse respiratory outcomes later in life8. PM10 and NO2 pollutants may be associated with reduced growth in forced expiratory volume (FEV1) and adverse effects including phlegm, asthma exacerbations, and increased hospital admissions9. In adults, exposure to air pollutants can lead to inflammation and changes in lung function, such as lower FEV1 and forced vital capacity (FVC) in the non-smoking population while also increasing asthma incidence and COPD prevalence9,10.
Pulmonary rehabilitation is a comprehensive intervention based on the thorough assessment of patients and subsequent implementation of individualized treatments. These treatments are designed to improve the physical and psychological well-being of patients with CRDs and promote long-term adherence to health-improving behaviors. They include exercise, education, and gradual behavioral change to adopt healthy lifestyles11. Pulmonary rehabilitation reduces the disability of people suffering from CRDs, promoting their independence and participation in education, work, and other life roles12,13.
Current evidence suggests that rehabilitation ‘needs to be brought close to communities as an integral part of primary healthcare to reach more people in need’14. The identification of epidemiological trends concerning CRDs and the assessment of rehabilitation needs may encourage public health practitioners to prioritize the implementation of pulmonary rehabilitation programs by extending the relevant services to primary health care. To this end, in this study, we aimed to identify trends in years lived with disability (YLDs) caused by air pollution-related CRDs both in Greece and worldwide, and assess estimates of the need for rehabilitation services during CRDs course.
METHODS
Data were explored from the 2019 Global Burden of Disease Study (GBD; https://vizhub.healthdata.org/gbd-compare/). GBD provides a systematic scientific review of published publicly available data on the incidence, prevalence, and mortality due to 369 diseases and injuries for both sexes in 204 countries and territories. GBD 2019 input data were drawn from censuses, household surveys, civil registration, patient registries, health service utilization, satellite imaging, and other sources15. Clinical information data included hospital admissions, outpatient visits (including general practitioners in primary health care facilities), and health safety data15. The selected parameters were: GBD estimate: risk factor, measure; YLDs, metric: rate, cause; CRDs, risk factor: air pollution; location: Greece and global; age: 50–74 years and 75–94 years; sex: male and female; annual rate of change: 1990, and 2019.
YLDs are expressed as years of healthy life lost due to a disability16. To estimate the number of YLDs for a particular cause in a given period, the number of cases in that period is multiplied by the average duration of the disease and a factor reflecting the severity of the disease on a scale from 0 (perfect health) to 1 (death).
YLDs are calculated from the formula: YLD = I × DW × L, where I is the number of new cases of a disease, DW is the burden of disability, and L is the average time a person lives with the disease before remission or death (years)17. YLDs are expressed per 100000 population. One YLD is equivalent to one full year of healthy life lost due to disability or disease18.
Estimates of CRD rehabilitation needs were assessed using the WHO Rehabilitation Need Estimator tool (https://vizhub.healthdata.org/rehabilitation/) which is based on GBD 2019 data to estimate the number of people with a lifetime health condition that could benefit from rehabilitation programs (prevalent cases). In total, the tool provides estimates for 25 diseases, and impairments amenable to rehabilitation14.
Extracted data were analyzed by location, gender, year, and age group (50–74 years; 75–94 years). IBM® SPSS® version 29 was used as the analysis software package. Data distribution was assessed using the Kolmogorov-Smirnov normality test. The Mann-Whitney test was used to determine significant differences in non-parametric data between two groups. Multiple regression analysis was employed to assess the effect of explanatory variables (location, age, sex, year) on YLDs caused by air pollutionrelated CRDs. For descriptive statistical analysis, continuous variables are expressed as mean ± standard error of the mean (mean ± SEM). The level of statistical significance was set to 5%.
RESULTS
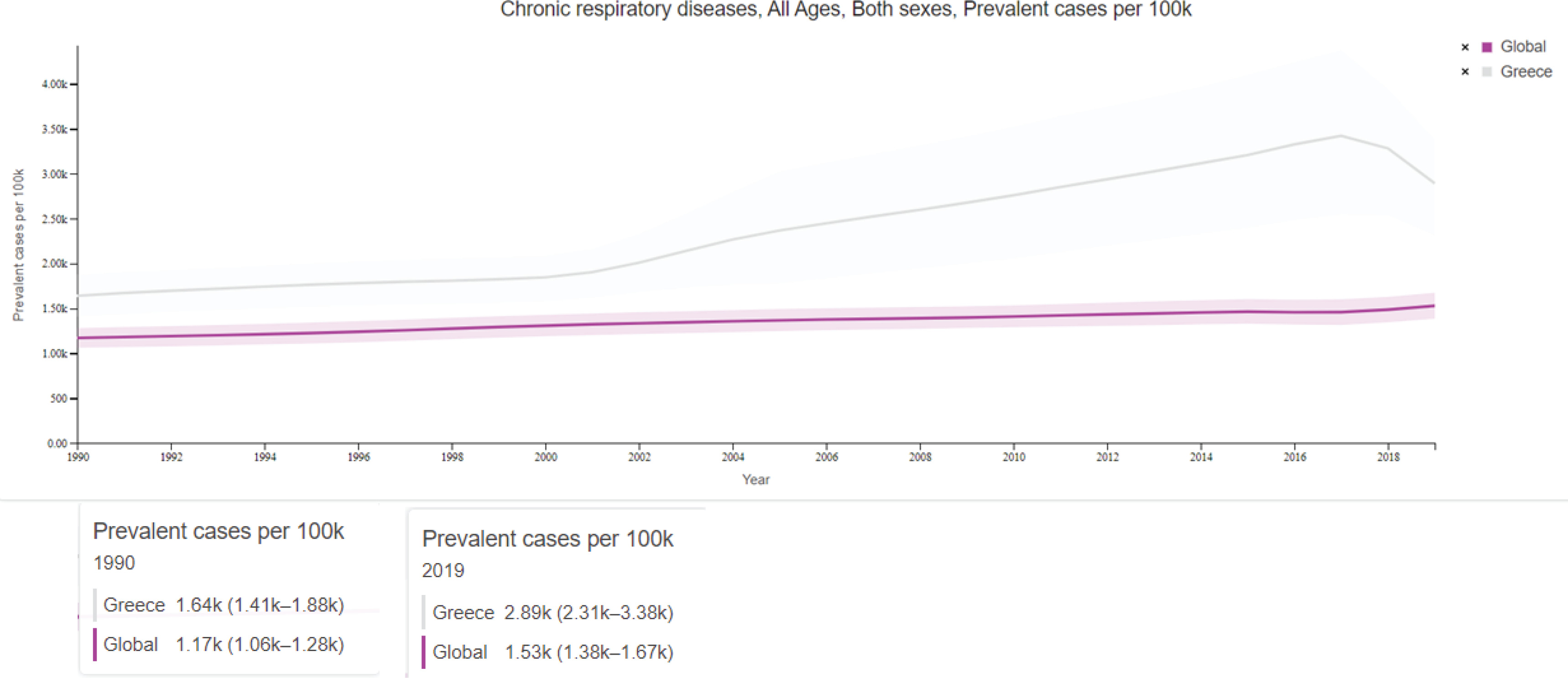
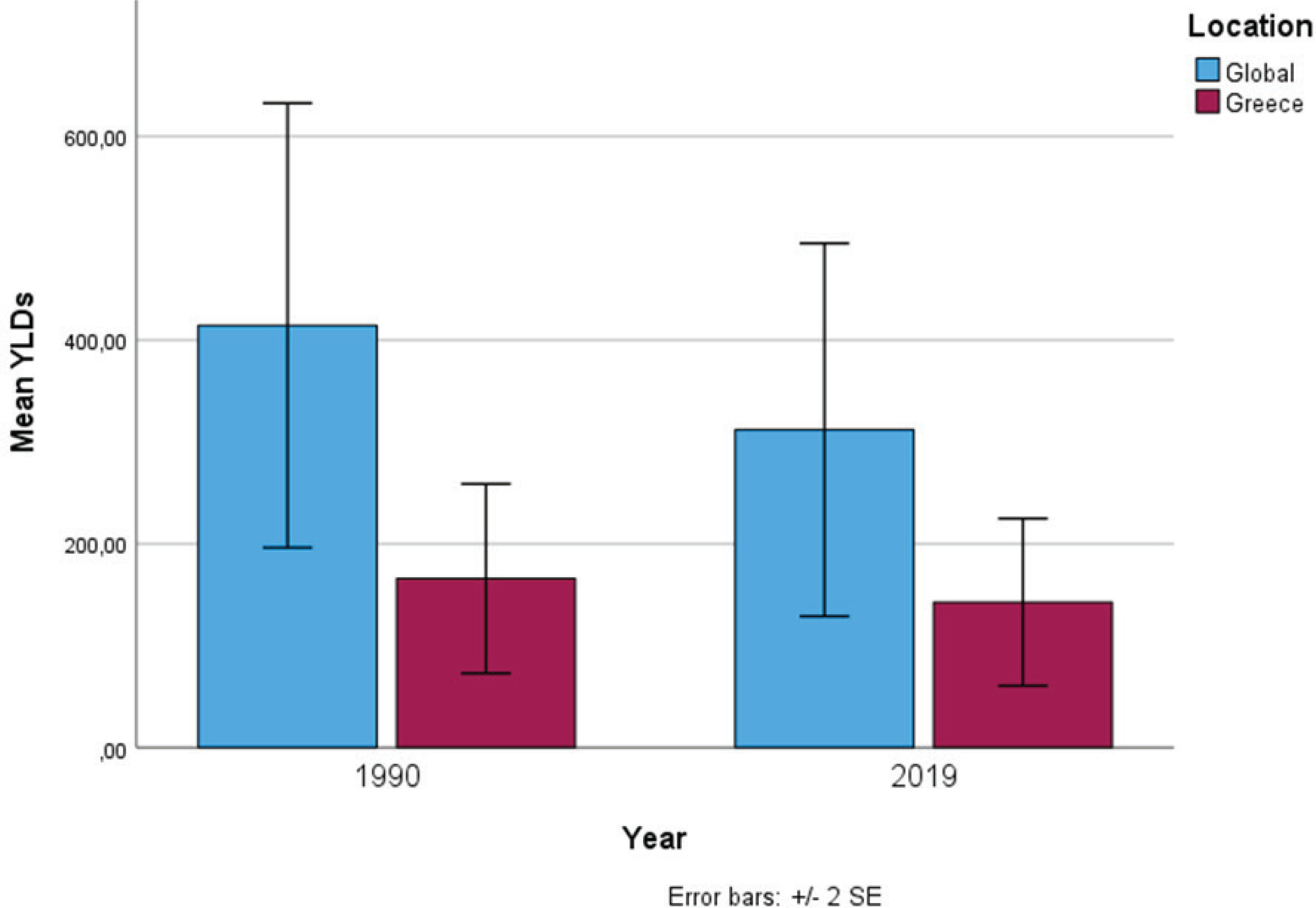
Investigation of the WHO Pulmonary Rehabilitation Needs Assessment tool showed that the prevalence of CRDs of non-specific etiology increased in 2019, compared to 1990, both globally and locally (Figure 1). However, YLDs caused by air pollution-related CRDs decreased in 2019 compared to 1990 both in Greece (142.66 ± 41.04 vs 165.85 ± 46.48) and worldwide (311.90 ± 91.57 vs 414.38 ± 109.07) (Figure 2).
Figure 1
Trends in the prevalence of CRDs of non-specific etiology in the Greek and global population during the years 1990-2019
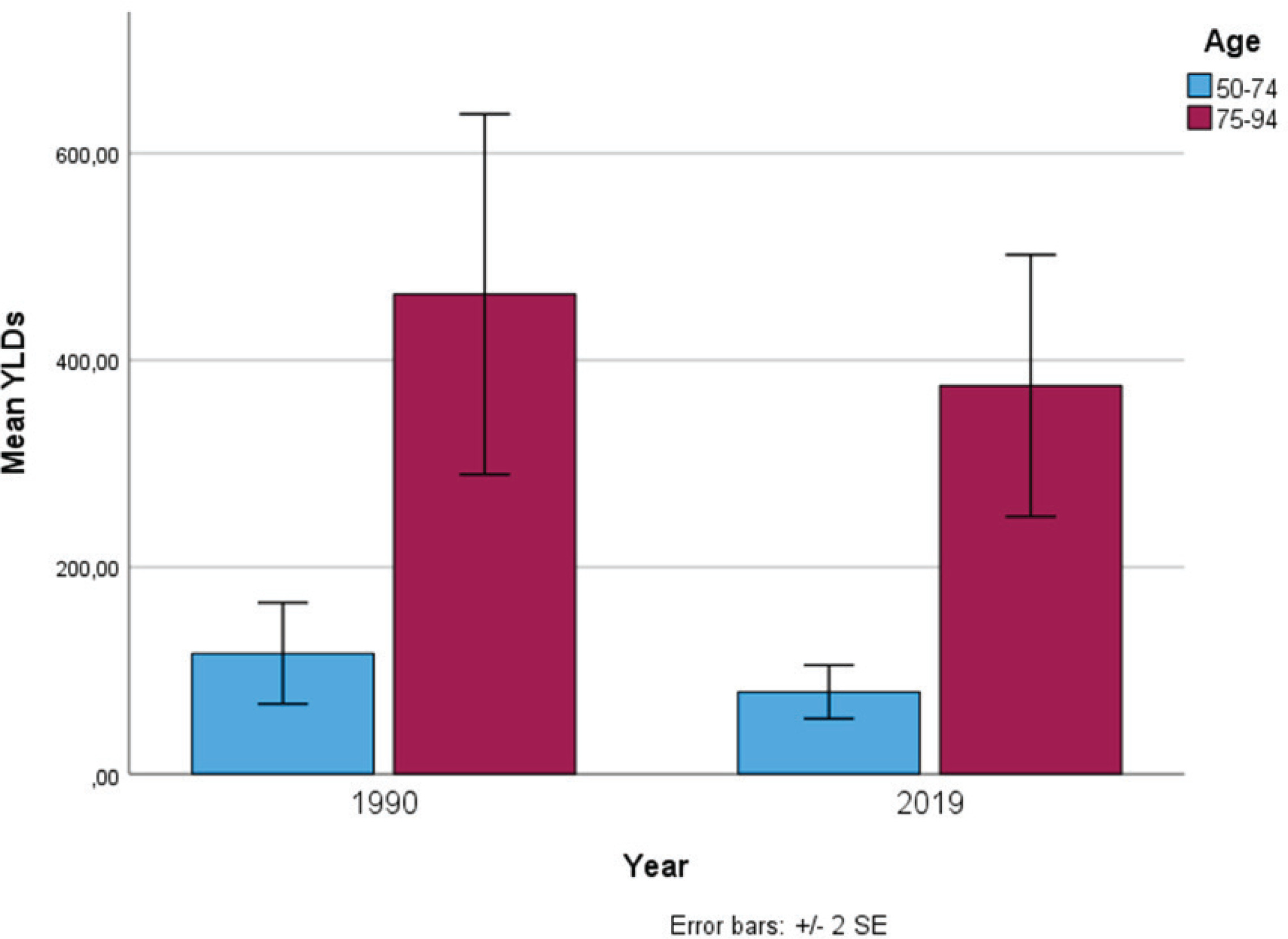
No significant differences in YLDs caused by air pollution-related CRDs were observed between sexes (p>0.05) both in 1990 and 2019. Mean CRD YLD values due to air pollution in the same years were significantly higher in the older age group (p=0.004) (Figure 3). Multiple regression analysis showed that YLDs due to air pollution-specific CRDs can be predicted based on location and age group (Table 1).
Table 1
Effect of multiple explanatory variables on YLDs caused by air pollution-related CRDs
DISCUSSION
Air pollution is a major threat to global public health. Nine out of ten people breathe air containing high levels of pollutants, above WHO guideline limits19. The updated WHO 2021 guidelines state that the safe concentration for PM2.5 is ≤5 μg/m3. Conversely, the higher the concentration, the higher the risk according to the following classification20,21: Low: 5–10 μg/m3, Moderate: 10–15 μg/m3, High: 15–25 μg/m3, Very high: 25–35 μg/m3 and Hazardous: >35 μg/m3. Of note, during the COVID-19 lockdown, in several urban areas there was a modest to major improvement in overall air quality because of the reduction in emissions from industrial and transportation sectors22,23. Under these conditions, people’s exposure to air pollutants decreased. As a result, there was a 60% reduction in hospital admissions due to asthma and COPD exacerbations both worldwide and in Greece23,24.
Air pollution is a cause and an aggravating factor for many diseases, particularly those of the respiratory system. CRDs affect the airways in the lungs and thus impair respiratory function1,25. Pulmonary rehabilitation is effective for patients with disability due to any CRD26. According to the American Association for Cardiovascular and Pulmonary Rehabilitation and the American College of Chest Physicians, pulmonary rehabilitation is beneficial for all patients with lung diseases, regardless of disease severity. After being developed for COPD, respiratory rehabilitation was quickly expanded to benefit other CRDs, including PAH and asthma27. Especially for COPD and asthma, there is strong evidence supporting that pulmonary rehabilitation is used across the age spectrum offering improved health outcomes in all cases28.
Thus, in the present study we aimed to identify trends in YLDs caused by air pollution-related CRDs both in Greece and worldwide and assess the need for the use of pulmonary rehabilitation services during the clinical course of these diseases. Globally, the number of deaths and the prevalence of CRDs of non-specific etiology increased in 2019 compared to 1990. CRDs are the third leading cause of mortality, following heart disease and cancer, accounting for 4 million deaths globally29. COPD is mainly responsible for this burden causing 3.3 million (range: 2.9–3.6) deaths worldwide29. In Greece, the prevalence of COPD has been estimated at 8.4% of the population aged >35 years30. Asthma has been the most prevalent chronic respiratory lung disease of the last three decades, with 262.4 million prevalent cases and 37 million (range: 29.6–45.9) new cases, affecting 8.6% of the general population in Greece29,31. Correspondingly, the prevalence of pneumoconiosis reached 3.1 million cases (range: 2.6–3.6)29. Studies have shown that population growth and aging have been the main causes of this burden29.
The rise in the number of YLDs due to CRDs of non-specific etiology in the last three decades was also remarkable, globally. Specifically, per 100000 population, there was an overall rate change of 59.4% (range: 51.9–67.9) for CRDs, 89.4% (range: 85.4–93.6) for COPD, 15.4% (range: 12.7–18.7) for asthma, 82.9% (range: 61.1–101.9) for pneumoconiosis, and 165.8% (range: 157.8–172.7) for other chronic lung diseases29. Regarding cause-specific (air pollution) YLDs due to CRDs, the results of this study show that they decreased in 2019 compared to 1990, both locally and globally. Nonetheless, as demonstrated by the WHO Pulmonary Rehabilitation Needs Assessment tool during the same time frame, the prevalence of CRDs increased globally and this increase was particularly evident in Greece. Therefore, it can be concluded that the need for pulmonary rehabilitation is high at the national scale.
WHO has set a target to reduce premature mortality due to CRDs by one-third, by 2030. Achieving this goal involves adopting sustainable development strategies to improve air quality29. Relevant policies aim to reduce traffic emissions and/or traffic-related air pollution (TRAP) concentrations from road mobile sources in urban areas32. Public health and social policy measures to reduce the burden of air pollution-related CRDs and respiratory infections include recommendations for individual protective measures (wearing face masks and regulating daily activity according to the air quality index1), tobacco-free environments, long-term urban planning, and distribution of vaccines for the vulnerable populations32.
The findings of this study suggest that environmental policy and air pollution control programs have contributed to reducing the burden of air pollution-specific CRDs. However, as the incidence and prevalence of CRDs continue to increase due to population growth and aging, these conditions will remain a major public health problem and high healthcare and pulmonary rehabilitation costs will be required in the future for their management. In addition, geographically targeted estimates should be assessed to reduce the burden of the above-mentioned diseases in specific regions33.
CONCLUSIONS
The findings of the present study suggest that environmental policy and air pollution control programs have contributed to the reduction of YLDs caused by air pollution-related CRDs. The results also show that the need for the use of pulmonary rehabilitation services is increasing both locally and globally due to the increase in the prevalence of CRDs of non-specific etiology which in turn is attributed to increased population ageing affecting both sexes. Therefore, CRDs remain a major public health problem, and high healthcare and pulmonary rehabilitation costs will be required in the future for their management.